
Abstract
Objective. The prospective efficacy of a future peripheral retinal prosthesis complementing residual vision to raise mobility performance in non-end stage retinitis pigmentosa (RP) was evaluated using simulated prosthetic vision (SPV). Approach. Normally sighted volunteers were fitted with a wide-angle head-mounted display and carried out mobility tasks in photorealistic virtual pedestrian scenarios. Circumvention of low-lying obstacles, path following, and navigating around static and moving pedestrians were performed either with central simulated residual vision of 10° alone or enhanced by assistive SPV in the lower and lateral peripheral visual field (VF). Three layouts of assistive vision corresponding to hypothetical electrode array layouts were compared, emphasizing higher visual acuity, a wider visual angle, or eccentricity-dependent acuity across an intermediate angle. Movement speed, task time, distance walked and collisions with the environment were analysed as performance measures. Main results. Circumvention of low-lying obstacles was improved with all tested configurations of assistive SPV. Higher-acuity assistive vision allowed for greatest improvement in walking speeds—14% above that of plain residual vision, while only wide-angle and eccentricity-dependent vision significantly reduced the number of collisions—both by 21%. Navigating around pedestrians, there were significant reductions in collisions with static pedestrians by 33% and task time by 7.7% with the higher-acuity layout. Following a path, higher-acuity assistive vision increased walking speed by 9%, and decreased collisions with stationary cars by 18%. Significance. The ability of assistive peripheral prosthetic vision to improve mobility performance in persons with constricted VFs has been demonstrated. In a prospective peripheral visual prosthesis, electrode array designs need to be carefully tailored to the scope of tasks in which a device aims to assist. We posit that maximum benefit might come from application alongside existing visual aids, to further raise life quality of persons living through the prolonged early stages of RP.
Export citation and abstract BibTeX RIS

Content from this work may be used under the terms of the Creative Commons Attribution 3.0 licence. Any further distribution of this work must maintain attribution to the author(s) and the title of the work, journal citation and DOI.
1. Introduction
Retinitis pigmentosa (RP) is one of the main causes of visual impairment and blindness in younger individuals as its onset is often during childhood or adolescence, affecting an estimated 1 in 4000 persons [1–3]. The condition involves gradual loss of photoreceptor cells, typically from the peripheral retina towards the macula. This causes progressive visual field (VF) constriction, from initial peripheral VF loss to eventual 'tunnel vision'. In some cases, central vision is affected and can result in profound blindness [4–6].
Retinal visual prostheses can restore rudimentary vision, bypassing damaged photoreceptors and electrically stimulating the surviving neural network directly, for example by activating the retinal ganglion cells (RGCs) whose axons form the optic nerve. Specifically, electrode array placements have been shown to be effective in five locations: sub-retinal [7, 8], epi-retinal [9, 10], intra-scleral [11], epi-scleral [12], and the supra-choroidal space [13, 14]. Upon electrical stimulation, artificial visual percepts, so-called phosphenes are produced and their position in the VF roughly approximates the location of electrode placement due to the retinotopic organization of the visual system. Current retinal prosthesis designs, with the exception of the epi-scleral approach [15], are implanted in close vicinity of the fovea to evoke artificial visual perception in the central VF [8]. Also, current prostheses have been designed for patients with no more than bare light perception. This restriction was due to the novelty of the implantation approach and to minimize jeopardy to residual vision from the procedure. It was reasoned that if there was minimal residual vision, the implant and its stimulation cannot do further harm [16].
These current selection criteria, however, constrain the development of this technology and exclude the majority of people with visual impairment from potential benefit. Retinal prostheses, found to work in principle in people with light perception only, should now be considered for less severe, but still debilitating forms of visual impairment. For example, the vast majority of people with RP may stay in the intermediate stages of the disease, retaining some peripheral or central vision. Stage classification according to residual VF is difficult due to the high inter-individual variability of the disease progress. However, longitudinal data suggest that around 4.6% of remaining VF is lost per year [17]; when residual vision is eventually confined to the central VF it takes approximately 9.4 years for half of the remaining VF to vanish [18]. This has been modelled as an exponential decline [19, 20].
It is therefore desirable to evaluate the feasibility and usefulness of bionic vision coexisting with residual vision with the aim of artificially extending the VF before vision deteriorates to light perception. This may assist to preserve quality of life for a significantly longer period of time in this larger cohort of people. While placing an electrode array in the vicinity of functionally useful retinal tissue requires significant caution, the documented rescue effect from electro-stimulation suggests that doing so may elicit a stabilizing [21] or even recovering [22] effect on residual vision and may minimize neural remodelling due to a lack of sensory input [23].
To our knowledge there has not been any study relating residual vision to prosthetic vision, nor on their simultaneous use. Peripheral vision loss is particularly detrimental in mobility tasks, affecting walking speed [24, 25], reaction times [26], spatial judgment [27, 28], and posture stabilization [29, 30], as well as increasing fear of falling [31]. VF constriction below 11–15° severely impacts efficient visual navigation [32, 33]. Also, mobility performance is closely tied to VF extent and to the central and lower mid-peripheral VF zones [32, 34]. However, the most effective placement and position of electrodes, and thus phosphenes, in the peripheral VF (i.e. outside the inner 30° of vision) remain unknown.
Presenting simulated prosthetic vision (SPV) to normally sighted participants, to evaluate the potential benefits of given electrode array layouts, has been shown to significantly reflect clinical findings [16]. Recently, performance in tasks such as reading [35], hand-eye coordination [36], object recognition [37], and mobility [38] has been evaluated for central phosphene layouts. Often, the angular field of view (FOV) of these layouts were similar to those of actual electrode arrays, for instance 20° in the Argus II [10].
Here, a study on mobility performance using peripheral SPV spanning up to 102° combined with central simulated residual vision (SRV) is presented to determine whether peripheral phosphene vision can aid residual vision to raise mobility performance in a range of navigational tasks. These results assist in determining optimal peripheral electrode form-factors, placement parameters and image processing strategies, as well as further guiding the research on the design of a peripheral prosthesis for non-end stage RP patients.
2. Methods
2.1. Simulation framework
2.1.1. Software components and image processing
To design a virtual outdoor obstacle course, a freely available computer game development engine (CryEngine 3.5.6, Crytek, Frankfurt, Germany) was used to create photorealistic environments, employing state-of-the-art, credible physics and artificial intelligence for enhancing meaningfulness of SPV research. CryEngine's open-source C++ code was modified and extended to integrate tracking of angular head motion from a head-mounted display (HMD). Thus, the participants' head scanning movements could be incorporated into the virtual scene gaze control (see Hardware specifications). The participants' position, walking speed, head orientation and motion, distance travelled, and collisions within the environment were recorded along with the corresponding timing of each these parameters.
Customized software for SPV and SRV written by the authors (MPZ, PM) in C#/C++ allowed for real-time capture of a video stream, image processing and subsequent presentation as phosphenized vision on a display. For this study, image workflow was as follows: the CryEngine environment was displayed on a computer screen with 1920 × 1080 pixel resolution at 75 Hz. The FOV of the scene was set to 160° × 90°. The screen content was continuously captured via a webcam at 640 × 400 pixel resolution and 30 frames per second (fps). Due to the difference in aspect ratios (16:9 versus 16:10), the webcam was positioned centrally to exactly capture the vertical extent of the screen, while discarding the far left and right portions, thus capturing a scene angle of 144° × 90°. The webcam stream was then processed by the SPV/SRV software (see 'SPV and SRV parameters' section) at 30 fps. Using the freeware Deskope [39], the processed image stream subsequently underwent up-sampling to 1280 × 800 pixel resolution and a series of image transformations (split-screen stereo rendering, distortion correction) to render to the stereoscopic display of the HMD at 60 Hz. Please see [40] for details. Since the HMD has a FOV of approximately 117.4° × 112.5°, as part of the rendering process, the SPV/SRV image was scaled to and centred within this FOV in order to ensure correct scene representation, and that the FOV of the scene part visible on the display matched its intrinsic FOV.
The webcam, being the component with the lowest resolution and sampling rate, determined the functional resolution of the final image on the HMD. Image capture and display at native HMD resolution would have been possible in theory; yet this would have introduced an extensive time delay within the series of already computationally demanding image transformations. The image processing and interaction between CryEngine and the HMD attributed to latencies less than 100 ms; a potential impact on task performance would have likely equally affected all experimental conditions. Figure 1 illustrates the hardware and software setup as well as the flow of data for image and motion processing.

Figure 1. Experimental setup. Participants navigated the CryEngine environment on PC 1 by head and controller motion. The scene on the screen of PC 1 was continuously captured by a webcam, relaying the image stream to PC 2. PC 2 was dedicated to mapping SPV/SRV to the scene image and performing distortion correction, scaling and rendering for adequate scene representation on the stereoscopic display.
Download figure:
Standard image High-resolution image2.1.2. Hardware specifications
The CryEngine environment was run on an Intel Core i7 PC with 24 GB RAM and 1 GB Nvidia GeForce GTX 550 Ti graphics card. Original CryEngine images were displayed on an Asus VS228N monitor (1920 × 1080 pixels, 75 Hz). A Logitech C905 webcam (640 × 400 pixels, 30 fps, minimal-distortion lens) fixated towards the monitor was connected to a second computer (Intel Core i7, 8 GB RAM, 1 GB GeForce GTX 650 Ti) for SPV/SRV image processing. The SPV/SRV image stream was displayed on an Oculus Rift DK1 (Oculus VR Inc., Irvine, CA, USA) HMD (1280 × 800 resolution, 60 Hz, 117.4 × 112.5° binocular FOV). Head-tracking data (yaw, pitch and roll) were acquired using the Oculus Rift's in-built gyroscope, with a sampling rate of 1000 Hz. The experimental participants navigated through the virtual environment with the aid of an Xbox Controller (Microsoft, Redmond, WA, USA) that was attached to the CryEngine computer over USB.
2.1.3. SPV and SRV parameters
Within the SPV/SRV software, multiple parameters such as phosphene size, separation and position could be freely adjusted by the experimenter as required for the combinations used in the study. Additionally, residual vision was displayed as circular tunnel vision of desired extent, adjusted to simulate the extent of retinal degeneration. Illustrative examples of the combined residual/phosphene images presented to the participants are shown in figure 2. For simulation of a fixed, central residual VF of 10° diameter, a black mask was applied to the displayed image stream, only omitting the circular central 10° portion. Along the boundary between SRV and mask, within the zone of 4–5° eccentricity, a transition zone of decreasing visual acuity (VA) due to progressing, partial photoreceptor loss was simulated by linearly increasing mask opacity from zero to maximum. Peripheral prosthetic vision was displayed in a hexagonally arranged mosaic of 100 simulated phosphenes in the inferior VF surrounding the SRV. An aim was to investigate sensible distributions of a limited electrode count similar to that of the central retinal prosthesis prototype of the authors, which reflects the current state of technology in implants which receive stimulation instructions from external vision processing units [41]. Three different array configurations were used in this study (figure 2):
- (1)'Higher-acuity layout'. Phosphene separation: 3°; minimum eccentricity: 10.6°, maximum eccentricity: 25.6°; horizontal/vertical extent: 51°/20.8° (figure 2(b))
- (2)'Wider-angle layout'. Phosphene separation: 6°; minimum eccentricity: 21°, maximum eccentricity: 51.2°; horizontal/vertical extent: 102°/41.6° (figure 2(c))
- (3)
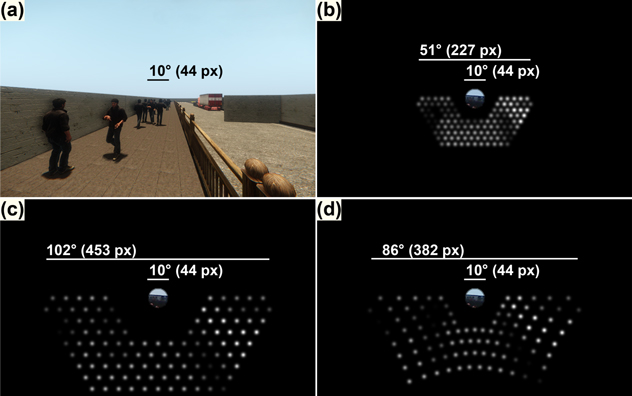
Figure 2. Peripheral phosphene layouts used in the study. Original image of the virtual scene presented on the HMD ((a); full vision condition); higher-acuity layout + residual vision (b); wider-angle layout + residual vision (c); eccentricity-dependent layout + residual vision (d). 'Residual vision only' condition is not shown. Scale bars depict the horizontal extent of SPV and SRV in degrees visual angle (°) and pixels (px) on the 640 × 400 pixel images processed by the simulation software.
Download figure:
Standard image High-resolution imageThis SPV/SRV model was to represent the perception experienced shortly after implantation of an electrode array, placed at a distance to functional photoreceptor tissue to not compromise residual vision. Therefore, a gap between SRV and SPV was introduced, its minimum extent (from 5° to 10.6° eccentricity in the higher-acuity layout) chosen to approximately equal the SRV radius itself.
Brightness of single phosphenes was determined by image luminance around their respective locations, using Gaussian-weighted filtering, which has demonstrated advantages over point sampling and regional averaging in visual fixation and smooth pursuit [43]. Filter width (σ value) was set to 66% of the inter-phosphene separation angle. This amount of overlap of Gaussian kernels has been shown to maximize information content of the prosthetic image [44].
Image clarity and the ability to discern between scene features are mainly determined by the range of luminance values present in the (phosphene) image, i.e. by scene contrast. Real-time 'contrast stretching' was applied to take advantage of the full dynamic range of the phosphene vision in low-contrast conditions [45]. Phosphene luminance levels were continuously normalized to cover the whole range of possible values, with the lowest luminance level found matched to a phosphene brightness of 0 (no phosphene, black), and the highest level set to 255 (brightest phosphene, white).
Each simulated phosphene was rendered using a Gaussian intensity profile (figures 2(b)–(d)).
2.2. Experimental design
Approval for this study was given under the authority of the UNSW Human Research Ethics Committee. Eleven participants having not previously experienced SPV were recruited (seven female, four male, mean age 25.1 ± 4.2 years) and invited to sit for nine weekly sessions. Session duration was limited to approximately one hour each to ensure participant comfort.
2.2.1. Experimental procedure and vision conditions
In each session, participants were seated on a chair adjusted to their comfort and fitted with the HMD which consequently occluded their regular vision, thereby ensuring that all visual input was exclusively from the HMD. Participants were then asked to navigate a photorealistic virtual obstacle course consisting of four tasks involving low-lying obstacle avoidance, circumvention of static and moving pedestrians and path following with the vision provided on the HMD. In order to keep ambient lighting conditions consistent across trials, CryEngine was configured to realistically simulate a cloudless, sunny day at 12.00 pm, including cast shadows (figure 2(a)).
The initial session was dedicated to training, and participants practiced the obstacle course with full vision of the scene shown on the HMD for one hour in order to get accustomed to controls and the task objectives. Data from this session was recorded but not included in the analysis. Recording of data presented in this study commenced from session 2.
Starting from the second session, participants were presented with five vision conditions depicting the virtual scene (figure 2), separated by 5 min breaks: (1) full vision of the virtual scene ('fv') presented on the HMD, central residual 10° vision only ('rv'), (2) residual vision plus 'higher-acuity' phosphene array ('rv + ha'), (3) residual vision plus 'wider-angle' phosphene array ('rv + wa'), and (4) residual vision plus 'eccentricity-dependent' array ('rv + ed'). At the beginning of each session, full vision was presented as a control to ensure proper functioning of software and hardware as well as participant comfort, and to determine session-specific preferred walking speed (PWS) [46]. Subsequently, the four reduced-vision conditions were applied in random order, together forming one test block (repetition).
Within one-hour sessions, participants were usually able to perform two repetitions of the scheme. Session duration was adjusted to allow completion of two repetitions given the participants' comfort and including short breaks. In cases where a participant was not able to perform two repetitions in one session, additional sessions were scheduled. Data acquisition for each participant was completed after 16 repetitions.
Participants were asked to navigate a virtual outdoor mobility course with the vision provided via the HMD. Participants were told to keep their eye gaze fixed on the centre of the display at all times (see section 4 'eye tracking and fixation'), but were able to use head motion to freely direct their gaze and scan the environment.
2.2.2. Virtual mobility tasks
The course consisted of four distinct tasks (figure 3).
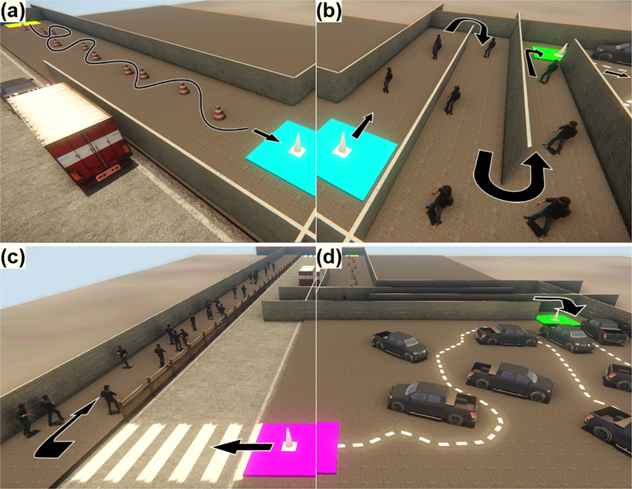
Figure 3. Virtual mobility tasks. low-lying obstacle circumvention (a); static pedestrian avoidance (b); moving pedestrian avoidance (c); path following (d). Lines and arrows depict the approximate movement sequence through the obstacle course from (a) through (b), (d), then (c).
Download figure:
Standard image High-resolution imageSafely navigating around low-lying obstacles is one of the greatest challenges for people with restricted peripheral VF due to RP [47, 48]. In the 'low-lying obstacles' task (figure 3(a)), participants were asked to walk along a sidewalk and to circumvent ten low-lying obstacles (road cones) in an alternating, slalom-like fashion. Emphasis was placed on avoiding collisions and correct alternation of side of crossing, and walking distance and time was to be minimized provided subjects were able to do so safely. Slalom movement required participants to perceive and relate proximal objects to their own position. This is analogous to daily situations where multiple obstacle positions have to be considered in order to estimate a safe walking trajectory. Before each run, road cone position was randomized within ±1.66 m perpendicularly, and ±0.83 m along the sidewalk, the range defined by the extent of the sidewalk.
The 'static pedestrians' task (figure 3(b)) included narrowing corridors and nine static pedestrians. Participants were asked to traverse the corridors while avoiding collisions with the pedestrians. To induce the necessity for continuous re-orientation and re-focusing on obstacles in the restricted environment, participants had to perform U-turns after every three pedestrians to further advance through the course. Before each run, pedestrian position was randomized within ±1 m perpendicularly, and ±5 m along the sidewalk, this range defined by corridor width and inter-pedestrian distance.
People with RP are largely concerned about 'moving about in crowded situations' [48]. In the 'moving pedestrians' task (figure 3(c)), participants were asked to walk a dynamic scene along a straight sidewalk, with 27 pedestrians moving along the length of the sidewalk. Participants were asked to avoid collisions. Movement decisions had to be continuously evaluated based on virtual pedestrian behaviour. Pedestrians were programmed to dynamically stop, evade and then choose a new path as soon as they came closer than 1.5 m to the participant, having a reaction time of 0.5 s. This was to ensure collisions occurred solely due to the participant walking into pedestrians rather than vice versa.
In real street scenes, paths are frequently highlighted by lines of variable visibility, which run not necessarily at right angles. Finding a path between obstacles, such as in a parking lot, is a common task. The 'path following' task (figure 3(d)) involved following a regularly intersected line on the floor as closely as possible and as fast as comfortable between large obstacles (cars). Eight cars were placed laterally to the path and in addition to being obstacles, further served as visual cover, preventing participants from overlooking the more distant line trajectory. On each iteration, one of five line-car arrangements of similar length was randomly chosen.
The four tasks were performed in the sequence a, b, d, c, resembling sub-sections of the continuous obstacle course.
Participants were able to adjust their velocity freely up to a maximum of 2.5 m s−1. This high upper limit was chosen to not restrict participants in case they felt sufficiently comfortable to navigate at higher speeds, yet without making navigation unstable due to abrupt movements.
2.3. Data acquisition and analysis
Throughout the experiment, the following raw data were continuously recorded and written to text files: participant position, speed, and collisions with any part of the environment. Data were imported into Matlab (R2014, Mathworks, Natick, MA, USA) for processing using custom software written by the author (MPZ) to determine motion and incidence variables, representing different objective measures of performance. In particular, these were: percentage preferred walking speed (PPWS), distance walked and time required to complete the tasks; and types of objects involved in collisions. Determining the number of collisions, repeated contacts with the same objects were counted multiple times if they occurred at least 0.5 s apart. In addition, the number of errors in the slalom course, i.e. deviations from an alternating left–right–left/right–left–right cone circumvention pattern, usually by missing or misjudging the position of single cones ('low-lying obstacles' task), was determined. Also, the average deviation in metres from the line ('path following' task) was acquired by continuously recording the Euclidian distances between participant position and the closest line coordinate, for each acquired data point. For the 'path following' task, since possible line trajectories differed in length, distance walked and time taken were normalized to a path length of 100 m.
PPWS has been introduced by Clark-Carter et al [46] and widely used to compare the effect of different aids in improving mobility performance. The PWS is the optimal speed that people with visual impairment would walk if their vision were fully restored. PWS has been originally determined for visually impaired people by letting them walk with the help of a sighted guide [46] or walking a straight unobstructed route [49, 50]. In the case of the present study the method of calculating this measure required adaptation as the participants all had normal vision so they were instructed to walk the same route with a full view of the visual environment on the HMD, i.e. one that was not restricted in VF by SPV or SRV, and their preferred speed assessed. The ratio of speed with the full view to the speed with the SRV or residual vision with assistive phosphene arrays was calculated. As compared to absolute walking speeds, PPWS allows participants to act as their own controls, normalizing data for differences in age, height, and physical fitness. In this study PWS was determined before each session, so normalizing for between-session variations in performance was established (see supplementary table 1 for observed PWS).
Processed data were then exported to SPSS 22 (IBM, Armonk, NY, USA) for statistical analysis. Approximate normality of the data subsets was assessed by visual inspection of Normal Q–Q plots [51] and histograms. Homogeneity of variance was ensured using Brown–Forsythe tests [52]. In case data followed an approximately normal distribution, parametric testing was chosen. Prior to investigating the data, we hypothesized that using assistive phosphene lattices would provide a significant difference in the means of the investigated variables as compared to plain residual vision, and that some layouts might be significantly better than others. A statistical test for pairwise comparisons was required. Due to the novelty of combining SPV and SRV and the variety of tasks and variables tested, potentially detrimental effects of assistive SPV as compared to SRV alone could not be ruled out. A two-sided test sensitive for effects in both directions was therefore chosen. Tukey honestly significant difference (HSD) tests with correction for multiple comparisons were performed [53]. SPSS required a preceding analysis of variance; here, a mixed model was chosen [54], factoring in the effects of vision condition and repetition (fixed factors) as well as controlling for subject (random factor). The Tukey HSD test is justified to be 'stand-alone' since it already protects against Type I errors [55–59]. A significance level of p < 0.05 was used. In case data deviated from a normal distribution, which was the case for the measures of task time, distance walked and deviation from line, the aligned rank transformation [60] was applied prior to Tukey tests. This method allows for a non-parametric analysis by applying ranks over the data set while a subsequent data alignment process simultaneously controls Type I error rate for multifactorial models. In the following section, graphs depict observed, non-ranked data (mean ± standard error) and statistical test results (asterisks, brackets) for each of the presented vision conditions. For PPWS, the values for 'fv' are not shown since they are implicit in the measure. In the supplementary tables, p values derive from the respective parametric or nonparametric test procedure applied.
3. Results
3.1. Effects of peripheral prosthetic vision on navigation around low obstacles
Participants made significantly less normalized errors using assistive phosphene with residual vision as compared to plain residual vision in the 'low-lying obstacles' task (figure 4(a)). This was the case for all three of the phosphene layouts in combination with 10° of residual vision. Errors counts were lowest using the wider-angle layout, followed by the higher-acuity layout and the eccentricity-dependent layout, as compared to plain residual vision.
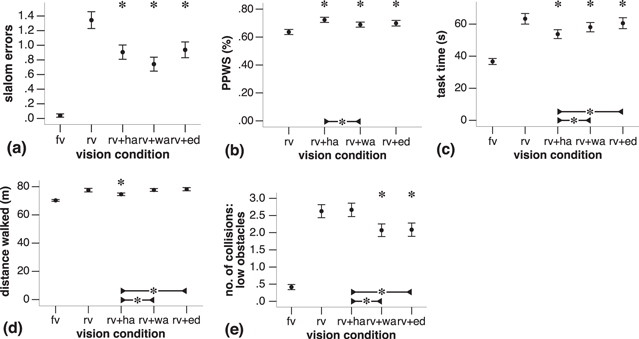
Figure 4. 'Low-lying obstacles' task performance as a function of vision condition (fv = full vision, as reference; rv = residual vision only; rv + ha: residual vision + higher-acuity layout; rv + wa: residual vision + wider-angle layout; rv + ed: residual vision + eccentricity-dependent layout). Slalom errors (a), percentage preferred walking speed (PPWS; (b)), task completion time (c), distance walked (d), and number of collisions with road cones (e). A single asterisk above a data point indicates a significant difference in means between the respective assistive phosphene condition and the 'residual vision only' (rv) condition, based on the mixed model and following Tukey HSD. Below, brackets connecting two data points indicate a significant difference in means between the two connected assistive phosphene conditions.
Download figure:
Standard image High-resolution imageMean PPWS, as compared to full vision was found to be significantly higher for all vision conditions that utilized phosphene lattices (figure 4(b)) than when plain residual vision was presented. The highest gains were found using the higher-acuity layout, followed by the eccentricity-dependent and the wider-angle layout. Also, PPWS using the higher-acuity layout was significantly higher than with the wider-angle layout.
The mean times needed to complete the task (figure 4(c)) were significantly reduced from residual vision only using the eccentricity-dependent layout, even more so with the wider-angle layout, and the fastest mean time was achieved with the higher-acuity array. The latter layout also afforded the participants with significantly improved performance over the other two layouts.
Notably, only when using the higher-acuity layout did participants walk significantly shorter distances than with plain residual vision (figure 4(d)). Paths were also significantly shorter than when using the other two layouts.
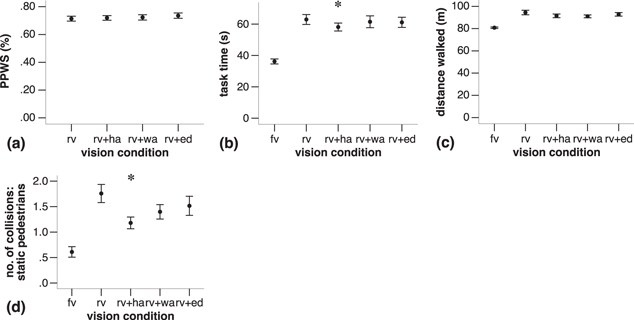
Figure 5. 'Static pedestrians' task performance. Percentage preferred walking speed (PPWS; (a)), task completion time (b), distance walked (c), and number of collisions with pedestrians (d). Data presented using the same conventions as in figure 4.
Download figure:
Standard image High-resolution image
Figure 6. 'Moving pedestrians' task performance. Percentage preferred walking speed (PPWS; (a)), task completion time (b), distance walked (c), and number of collisions with pedestrians (d). Data presented using the same conventions as in figure 4.
Download figure:
Standard image High-resolution image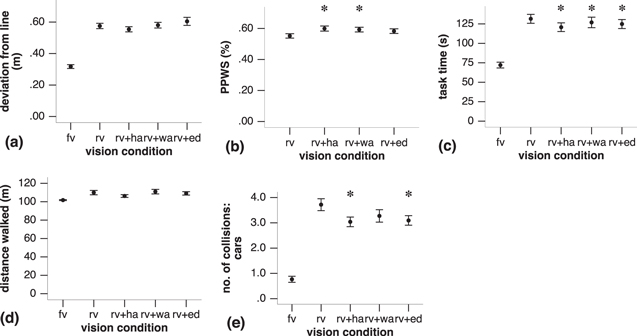
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Figure 7. 'Path following' task performance. Deviation from the line (a), percentage preferred walking speed (PPWS; (b)), task completion time (c), distance walked (d), and number of collisions with stationary cars (e). Data presented using the same conventions as in figure 4.
Download figure:
Standard image High-resolution image{kind=link}
Contrasting the faster pace and shorter trajectories when using the higher-acuity layout, participants experienced a significantly lower average number of collisions with the ten low-lying obstacles only when using the wider-angle and eccentricity-dependent layouts, as opposed to both plain residual vision and the higher-acuity layout. See figure 4(e). Supplementary tables 2 and 3 show statistical test results for all variables measured in this task as well as observed mean values and standard errors.
3.2. Effects of peripheral prosthetic vision on navigation around static pedestrians
Walking speed, completion time, distance walked, and collisions in the 'static pedestrians' task are shown in figures 5(a)–(d). Average task time using the higher-acuity layout was significantly reduced as compared to plain residual vision (figure 5(b)). Participants also incurred significantly fewer collisions with static pedestrians using the higher-acuity layout (figure 5(d)), than with plain residual vision. See supplementary tables 4 and 5 for statistical test information as well as observed means and standard errors for all variables recorded for the 'static pedestrians' task.
3.3. Effects of peripheral prosthetic vision on dynamic navigation around moving pedestrians
Walking speed, completion time, distance walked, and collisions in the 'moving pedestrians' task are shown in figures 6(a)–(d). Moving along a sidewalk with 27 moving pedestrians, reductions in PPWS using peripheral phosphene lattices as compared to plain residual vision (figure 6(a)) were statistically significant for the wider-angle layout. In supplementary tables 6 and 7, outcomes for all statistical tests as well as observed means and standard errors for the 'moving pedestrians' task are listed.
3.4. Effects of peripheral prosthetic vision on locating, tracking and following a path
Deviation from the line, walking speed, completion time, distance walked, and collisions in the 'moving pedestrians' task are shown in figures 7(a)–(e). Participants were able to significantly increase PPWS with peripheral phosphenes using the higher-acuity and wider-angle layouts (figure 7(b)). With all phosphene layouts augmenting residual vision, significantly less time was needed to reach the end of the path (figure 7(c)). Participants were able to significantly reduce collisions with the cars along the path using higher-acuity and eccentricity-dependent layouts (figure 7(e)). See supplementary tables 8 and 9 for statistical test outcomes as well as observed means and standard errors for all variables recorded in the 'path following' task.
4. Discussion
4.1. Assistive peripheral prosthesis as a supplement to other aids?
The benefits of the proposed assistive prosthesis layouts were found to be task-dependent, which also applies to many other mobility aids.
4.1.1. Low-lying obstacles
With any of the presented phosphene layouts, participants gained capacity for well-directed circumvention of small, low-lying obstacles. In doing so, the higher-acuity placement of phosphenes allowed for better efficiency in terms of speed, task time and walked distance than plain residual vision or the other layouts. On the other hand, wider-angle or eccentricity-dependent layouts allowed the participants to avoid collisions more effectively than with plain residual vision or the higher-acuity layout. Showing that road hazards can be perceived earlier and from a distance using peripheral phosphenes highlights a useful application for an assistive prosthesis.
4.1.2. Static pedestrians
Navigating around static pedestrians, the benefit of assistive peripheral phosphenes was less pronounced. Reports indicate that avoiding bumping into head-high objects or people is a less difficult task for people with RP than circumventing low-lying objects [48]. If the task of avoiding static pedestrians in a narrow alleyway was naturally easy for our participants, then there may be little room for improvement hence no further significant improvements regarding speed or distance walked were registered. Consistently, PPWS for plain residual vision was relatively high, and participants using this condition increased walking distance by on average only 18% with regard to full vision.
4.1.3. Moving pedestrians
Assistive phosphene vision did not significantly improve performance compared to plain residual vision when navigating the sidewalk with a high number of moving pedestrians. Commonly, an increase of speed as a function of VF extent has been reported [24, 25, 61]. So why did participants choose to walk more slowly with the wider-angle layout than with plain residual vision? Raised cognitive load may explain the findings. In a previous SPV study on street scenes, increasing the number of dynamic elements raised decision times and demanded more visual information to proceed [62]. It similarly suggested that dynamic environments require more visual information to make safe choices than static setups. We posit that the wider-angle layout delivered a higher number of simultaneously perceived dynamic elements without providing sufficient detail for interpretation. Furthermore, the presented narrow path limited the use of wider-angle vision and possible directions for evasive behaviour. Future studies should determine situations when additional phosphenes may be more useful. For example, it may assist in detecting the approach of up to three pedestrians, considering people's natural ability to track trajectories [63], or in wider spaces such as public squares or metro stations.
4.1.4. Path following
Assistive peripheral phosphenes aided confidence in tracking a partially obstructed visual cue (line), and following the given irregular, indicated path. Movement speed was increased and task time was decreased with assistive peripheral phosphenes. VF extension possibly helped to keep the path trajectory in sight, allowing for swifter movement. The already small deviation from the path with plain residual vision was not significantly further reduced with assistive phosphenes. This is consistent with results from driving experiments indicating that lane keeping ability is not significantly affected by VF loss [64].
Altogether, a given prosthesis design might only be able to address a portion of the scenarios considered particularly challenging [48]. Conceivably, a visual prosthesis will be used in conjunction with other mobility aids to fill existing gaps in the assistance scheme, rather than being an all around tool. For example, a mobility cane may serve to raise awareness of visual impairment and evasive behaviour in bystanders well in advance. This would allow the patient to perform efficient wayfinding using the prosthesis while clearing the path and minimizing unexpected pedestrian behaviour. Such uses could be further explored with the assistance of orientation and mobility and other low vision rehabilitation professionals.
4.2. Predicting benefit of assistive phosphenes
Interestingly, the lower the PPWS when using residual vision only, the more pronounced the beneficial effects of assistive phosphenes. In the 'low-lying obstacles' (64% PPWS) and 'path following' tasks (55% PPWS) performance was improved by several phosphene layouts across multiple measures. In the 'static pedestrians' task (71% PPWS) performance was only improved by the higher-acuity grid, and not at all for 'moving pedestrians' (89% PPWS). 'Baseline' PPWS values falling below a certain threshold (here, around 70%) might identify candidate tasks for assistive prosthetic vision.
On each start of the obstacle course—within the 'low-lying obstacles' task—there might have been an adaptation period of decreased performance. In case adaptation to the visually most restricted SRV-only condition had been particularly pronounced, its performance detriment could have been overrated. This might have exaggerated benefits of assistive phosphenes for this task. Randomization of task order will be introduced in future studies to counteract such effects.
4.3. VF versus VA trade-off
After identification of candidate scenarios for a peripheral prosthesis, a trade-off between electrode array resolution and the covered VF angle will have to be established. Providing equally higher-acuity vision across a larger VF extent by increasing electrode count is currently not possible due to technical and physiological constraints [65].
Higher phosphene resolutions benefitted navigation under SPV [38, 62, 66]. Likewise, VA contributed to walking and mobility under RP. However, these reports are in line with other researchers stating that VF extent more strongly predicts mobility performance than VA [24, 25, 34, 49, 67–69]. FOV up to 70° [32] can be beneficial for mobility performance. Previous consideration of a wide-field prosthesis [70] reflects this. Studies particularly emphasize the importance of certain VF areas such as the central 37° and the inferior areas for mobility and fall prevention [34, 61, 71, 72]. In self-reported surveys, the central 5° as well as the central 10–30° best predicted self-reported vision-related activity limitations in mobility [73].
Targeting low-contrast scenarios, covering these crucial VF areas with a certain level of VA might produce highest benefit, as reflected by the higher-acuity layout. At higher contrast, maximizing VF does not necessarily improve all aspects of mobility: when circumventing low-lying obstacles, collisions were reduced at the expense of speed. Rather, different goals in accomplishing the respective task are balanced based on the provided visual information.
4.4. Role of optic flow
Previous research has shown the role of optic flow—based movement strategies for walking and in peripheral VF loss [27, 74]. In the higher-acuity phosphene layout, the gap between residual and phosphene vision was smaller, improving optic flow between the two modalities. In the wider-angle and eccentricity-dependent layouts, optic flow was instead available more peripherally, permitting a continuous perception of obstacles during crossing. Potentially, optic flow in the central FOV plays a role for choosing movement speed, while peripheral optic flow is important for judging safe distances when passing by objects. This might explain the lower low-lying obstacle collision count with more eccentric phosphenes. Ultimately, despite the aforementioned benefits of higher-acuity layouts, prevention of incidences might be more important than task completion speed, implying that visual angle should be kept at a maximum.
Foreseeing this conflict, the hybrid, eccentricity-dependent layout featured a smooth transition of resolution. Yet, results did not always favour this geometry. We hypothesized that, due to its higher complexity, learning might have not been completed during the course of the study. Regression analysis however disproved this assumption: on average across subjects, from within the second half of the study (repetitions 9–16), slopes of best-fit lines were not significantly different from zero across all variables, conditions and tasks. Alternatively, the distribution of phosphenes in the VF might have been non-optimal. Potentially, recipients rather favour a clear split between a number of central, high-acuity phosphenes for detecting finer details, supported by a range of high-eccentricity, low-acuity phosphenes catching movement or contrast differences in the periphery.
4.5. Simulations as an approximation to clinical conditions
The phosphenes displayed in simulations like the one presented are idealized representations of the percepts feasible in an actual implant. Guidelines for adequate simulation in order to address this discrepancy have been proposed previously [75], to which we adhered. Even idealized representations can have close correlation to clinical findings [16]. Nevertheless, the achievable clinical benefit of peripheral electrode arrays might be less pronounced than reported here. For instance, with ten discernable phosphene luminance levels reported clinically [9], the number of levels in this simulation represents a best-case scenario.
Similarly, virtual and real-world navigation strategies might differ. In the latter, collisions potentially have serious consequences; collision avoidance is likely favoured over speed. Follow-up studies should centre on the how deviations from ideal phosphene and real-world scene perception influence the achievable benefit.
4.6. Eye tracking and fixation
One limitation was that no monitoring was performed as to whether participants complied to fix their gaze at the centre of the display at all times. Eye tracking for gaze-locked viewing has been used previously in SPV [76–78]. However, attaching an eye-tracking device in a suitable angle between the tightly fitted HMD and the participant's eyes was infeasible. Further, the more extensive phosphene layouts covered a major portion of the available FOV. Constantly repositioning the SPV and SRV on the display at the centre of gaze direction, larger gaze angles would have resulted in cutting off phosphene fields of these layouts at the edge of the display. Similarly, restricting user eye gaze within certain angles to prevent this would not have benefitted realism. Lastly, at notable display latencies, such as present in our setup, large saccades are reportedly difficult to track [77].
The SRV, the highest-resolution part of the VF, would have been predominantly directed to the most salient scene features, and thus largely hold participant attention and fixation, as these are linked [79]. Within these 10° of SRV, it is imaginable that participants applied saccades to centre gaze on salient features. This might have increased performance similarly across all presented conditions. In case saccades elevated SRV-only performance more strongly and thus diminished the difference to the SRV + SPV conditions, the benefits of peripheral SPV reported here might have been more pronounced with gaze locking applied.
Wandering of the gaze to the SPV might as well have occurred, possibly lowering performance with assistive phosphenes, due to the predominantly lower visual information obtainable relative to the residual vision.
We chose to retrospectively characterize the role of eye tracking. Though software-based, quantitative eye tracking was not feasible, lateral recording of eye movements for qualitative analysis was possible and thus performed in a separate (unpublished) study—on three independent participants while being presented the wider-angle and higher-acuity layouts. Instead of displaying SRV, participants were asked to fixate a white pixel in the centre of the display while performing the 'low-lying obstacles' task. Even without the high-acuity central stimulus, we found that subjects typically fixed their gaze reliably and did not deviate in a coordinated fashion. Nevertheless, future studies will implement eye tracking, which will be less likely to underestimate benefit provided by assistive phosphene vision.
4.7. Implications of early implantation and relationship to centrally implanted prostheses
After implantation, the residual VF will continue to constrict; therefore gap size will further increase, which will also impact on optic flow. Eventually, residual vision will disappear. Since central VF is important, keeping the initial gap between residual and prosthetic vision as small as possible might be advisable. Ultimately, a safe implantation distance of an electrode array not compromising viable photoreceptor tissue will have to be determined. Supra-choroidal prostheses are particularly suitable in this scenario.
This study focused on the evaluation of the benefits of early implantation. Basically, explantation of a peripheral supra-choroidal array in favour of a central array following the disappearance of central residual vision is possible [80]. However, since any surgical procedure carries risks, peripheral designs should maintain a comparable mobility performance to that of a later implanted central array. Given the considerable time span between early implantation and complete central vision loss, it is imaginable that recipients will learn to use peripheral phosphenes to the same effect as central ones. Furthermore, due to the anatomical displacement of target RGCs in the centre of the fovea, elicitation of phosphenes in the very central VF is infeasible. Any implanted 'central' array therefore would likely be offset peripherally to a certain distance, diminishing its advantage in providing 'higher-acuity' central prosthetic vision.
4.8. Strategies for optimizing perceptual quality
Apart from optimizing electrode array geometry, alternative techniques can improve the perceptual quality of prosthetic vision. Head scanning, in particular increased scanning velocity, can facilitate detecting fine details [81]. Training participants to apply goal-directed head scanning strategies might be particularly useful when the distance between phosphenes in a wide-field prosthesis is relatively high.
Alternatively, implementation of image processing algorithms which detect and emphasize salient features for display is a viable approach to maximize the information content of a low-resolution, wide-spread prosthetic display [76, 82–84]. The authors' external vision processor in development for the current iteration of visual prosthesis is capable of a range of real-time processing steps such as edge detection and depth mapping between image capture and display [85].
5. Conclusion
The outcomes of this study indicate that a peripheral prosthesis has the potential to extend the benefit of bionic therapy to years before the disease stage is reached when current central prostheses are implanted. Spreading the available number of phosphenes over a wider area in the lower VF has been shown to be beneficial for detecting and avoiding compact, low-lying obstacles. Conversely, concentrating phosphenes in the more central lower VF around the residual vision was beneficial when navigating narrow environments, For dynamic scenes involving motion, peripheral phosphenes might only be helpful at low to medium scene complexity, unless resolution can be increased.
The insights gained can accelerate decisions on electrode layouts and target tasks for peripheral prostheses. A decision whether the magnitude of benefits reported here is large enough to justify the risk of prosthetic implantation can however not be made at this stage. This will ultimately depend on judgments, bolstered by the outcomes of on-going clinical trials, whether the percepts elicited and improvements found in this study can be reproduced by actual prosthetic stimulation, and whether the reported benefit might be further increased by combined use with existing visual aids, image processing and neuroplasticity associated with longer-term training. Still, like in central prostheses before, a definite answer will only be obtained after the first implantations of prototypes, choice and judgement lying with health professionals and ultimately with the recipients.
On the path to implantation, SPV can only be the first step. It can help to infer from promising phosphene layouts to actual electrode array geometries. Subsequently, manufacturing techniques established for current visual prosthesis designs will have to be re-applied to re-shape current retinal implant technology to the layout desired. Consequently, the safety of implantation of a peripheral array has to be evaluated in vitro and in vivo. Fortunately, other parts of the prosthesis such as micro-stimulator chips, wireless telemetry and external vision processing only require minor adaptations.
While many open questions have to be addressed, a promising approach has been introduced to extend the benefits of bionic therapy to a larger cohort of visually impaired, and over a larger period of time. Since progression of VF constriction in RP is highly variable, it will be advisable to consider individual patient history in order to shape electrode designs to individual patterns of retinal degeneration, and to evaluate individual benefit by a given design.
Ultimately, every vision aid has its intrinsic limitations. Combining established vision aids such as canes and guide dogs with a peripheral bionic therapy might attenuate these individual limitations and thus reduce the challenges low vision patients face in daily life.
Acknowledgments
This research was supported by the Australian Research Council (ARC) through its Special Research Initiative (SRI) in Bionic Vision Science and Technology grant to Bionic Vision Australia (BVA).
Footnotes
- 3
Phosphene separation (°) was determined by the polynomial y = 1.3*(2.4 + 0.058x + 0.022x2 – 0.000 22x3), where x is eccentricity. This is an adaptation of the polynomial describing the eccentricity-dependent increase in midget cell receptive field size in Dacey et al [42], y = 2.1 + 0.058x + 0.022x2–0.000 22x3. Offset was increased and a stretch factor of 1.3 applied to achieve a horizontal layout diameter comparable to the wider-angle layout, while maintaining a small gap between residual and phosphene vision comparable to the high-acuity layout.